A Black Sacramento resident thought HIV would kill him. What he learned could save lives
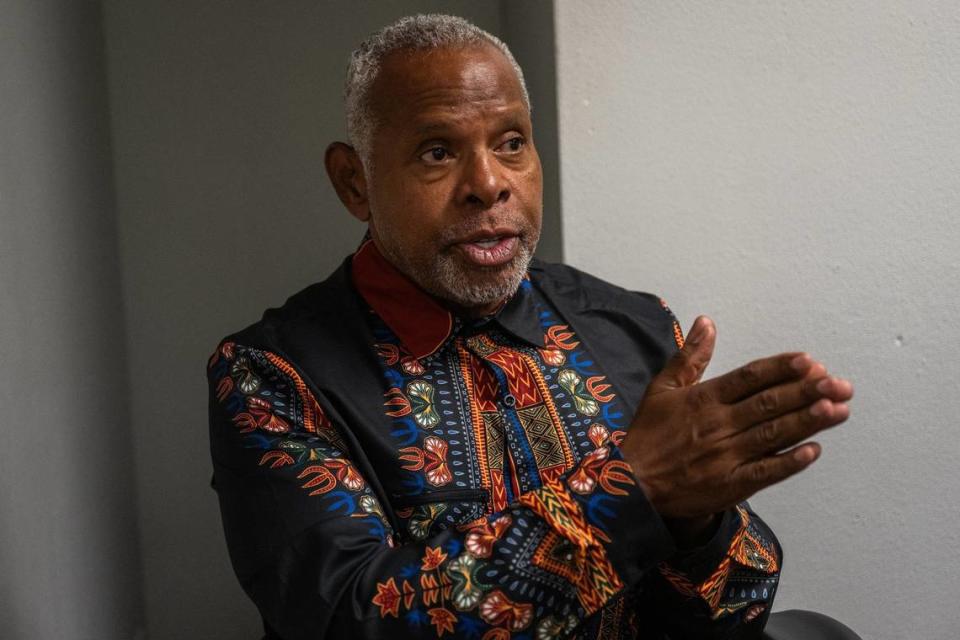
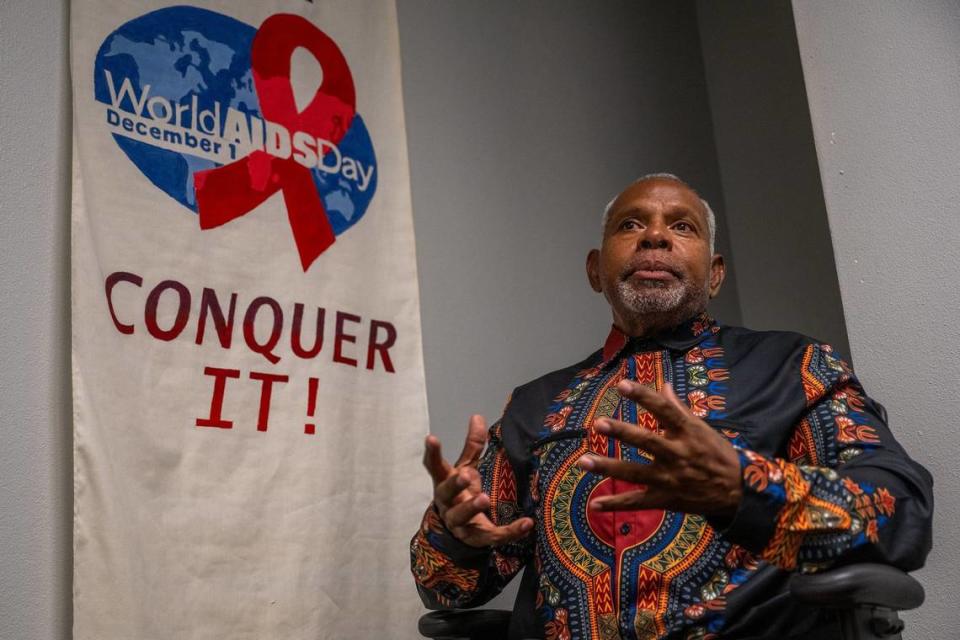
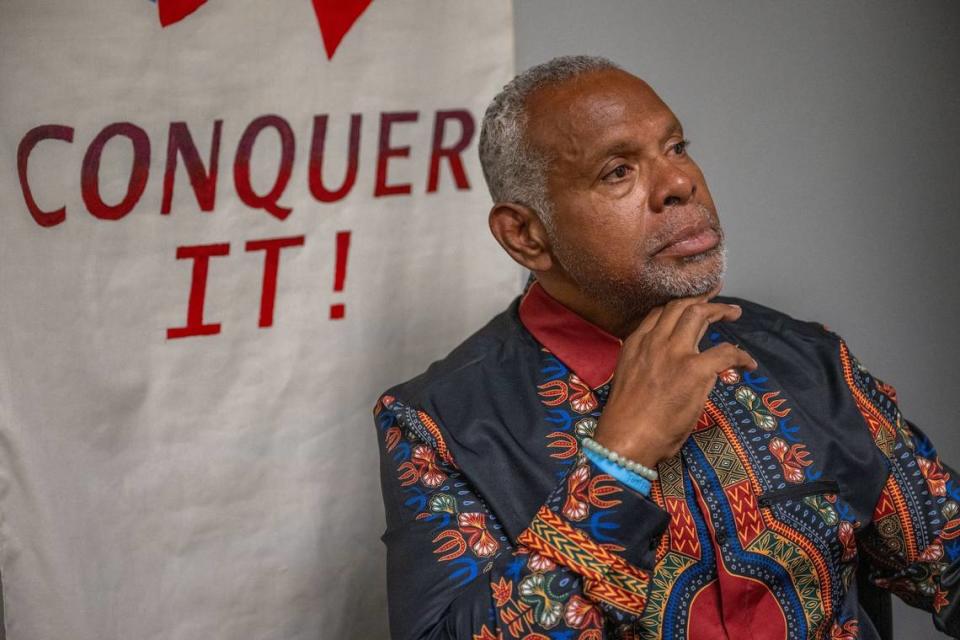
Sacramento resident MacArthur Flournoy has lived with HIV since 1988, though a nurse at the time told him that he would likely die within two years.
Flournoy is African American. He’s a grandfather of four. At age 64, he still lives a full, busy life.
The human immunodeficiency virus, best known by its acronym HIV, is no longer a death sentence, Flournoy said, but far too many people still believe it is.
The truth is that, if African Americans living with HIV take antiretroviral therapy, or ART, not one of them has to die from complications related to HIV, Flournoy and other HIV experts said.
Daily pills or a long-lasting injection of drugs known as PrEP, or pre-exposure prophylaxis, will keep them from contracting or transmitting HIV when taken as prescribed, Flournoy said.
And multiple studies have shown that, if people suspect they have had sex with someone who has HIV, they can avoid getting the disease if they start taking a 28-day prescription of PEP, or post-exposure prophylaxis, within 72 hours of contact.
Think you can’t afford HIV medications? They’re free to the poor at many clinics and are covered by Medicaid, Medicare and health plans. Many clinics also offer free confidential or anonymous testing.
Despite these medical advances and the defrayed costs, Black residents represented a disproportionately high number of Sacramento County’s newly diagnosed HIV cases — nearly 25% for the 10-year period ending in 2021 — though they account for roughly 9% of the population.
Nationally, African Americans represented 39% of newly diagnosed HIV cases in 2022 but only accounted for 14% of PrEP users in 2023, according to Emory University’s AIDSVu website. Records at the Sacramento County health clinic at 4600 Broadway show Black people currently make up 12% of the 89 people in that facility’s PrEP program. County health providers are not required to report PrEP usage.
By contrast, the AIDSVu site shows that white Americans made up 24% of new HIV cases in the US in 2022 and 64% of PrEP users in 2023. About 62% of Americans identify as non-Hispanic white.
Earlier this month, a committee of leading health equity researchers, including Dr. Ruth Shim of the University of California, Davis, cited the troubling rates of newly diagnosed HIV infections among Black people and called for more research on how to increase awareness and use of testing, preventative therapies and treatments.
The committee addressed the HIV disparities as part of an exhaustive examination of health inequities in the US health care system, conducted by the National Academies of Sciences, Engineering and Medicine.
Last year, the California Task Force to Study and Develop Reparation Proposals for African Americans also touched on the topic, decrying the disproportionately high loss of Black lives to HIV and AIDS since the 1980s and calling for health-based reparations to better control the spread of the disease.
“African American gay and bisexual men are infected by HIV more than any other group in the United States today and have the highest HIV death rate,” the task force noted. “Longstanding inequities in access to and delivery of healthcare to African Americans has led to this disparity.”
Flournoy, who identified as bisexual earlier in his life, vividly recalled how he found out that he had HIV. He had developed a cyst on his back, and it had become infected, so his primary care doctor sent him to a surgeon to remove the damaged tissue.
“He did the procedure with the cyst, and he said in a very matter-of-fact way, ‘Well, you know you’re HIV-positive, don’t you?’” Flournoy said. “Then his nurse came into the room and said, ‘You have two years to live.’”
‘I thought that was the end of me’
That was how Flournoy learned he had HIV. He choked up as he shared the memory: “I really thought that was the end of me.”
He had been married to a woman for about three months, he said, but prior to his union, he’d had sexual relations with men. He got his HIV diagnosis while his wife was in graduate school in Pennsylvania, but they returned to their native Los Angeles after she finished her coursework.
Flournoy said he feared that his HIV would progress to AIDS and that he would develop Kaposi’s sarcoma, a cancer that forms lesions on the face, arms and legs. So, about six years later, after he and his wife divorced, he moved to the Bay Area because he didn’t want his mother to see how the disease would ravage his body.
He planned on dying there, he said.
But Flournoy never developed AIDS. In 1987, the US Food & Drug Administration approved the first antiretroviral medication to prevent or treat HIV/AIDS: AZT, or azidothymidine, and Flournoy eventually started taking it.
He began to educate himself on AIDS research, and he began to use this knowledge to ask better questions of his doctors.
“You reach a point where you not only decide, ‘I want to live,’ but you get to decide how you want to live and what I learned is that I don’t have to settle for a life that is less than what I want,” Flournoy said, “and so I got proactive around partnering with health care. I got proactive around my mental health. I got proactive around my resources.”
Knowing your HIV status is the first step toward taking control of your life, Flournoy said, and it’s best to know before opportunistic infections gain the upper hand in your body.
In 2019, the U.S. Department of Health and Human Services set two ambitious goals: Reduce new HIV infections by 75% by 2025 and by 90% by 2030, but as of 2022, the department reported, the estimated number of newly diagnosed HIV cases had declined by only 12% since 2018.
In a statement sent to The Bee, the US Centers for Disease Control and Preventionexpressed concern about the nation’s ability to meet the 2030 goal, saying efforts must be accelerated.
Rhonda Smith, the leader of the California Black Health Network, said she has been working for some time to eradicate these sort of deep health inequities, but now, she doubts that will be possible in her lifetime.
Racism and implicit bias often affect the quality of care that brown and Black people receive from their providers, Smith said, and even when terrific new policies are undertaken, she said, the implementation falls short.
She’d like to see more studies to determine the best practices to get communities of color to adopt new treatments or health policies, she said, and medical schools and other graduate programs must do a better job of educating students on how racial biases among providers are hurting patient outcomes and leading to higher rates of mortality for Black people.
Leading health equity researchers detail plan of action
In the report to the National Academies, “Ending Unequal Treatment: Strategies to Achieve Equitable Health Care and Optimal Health for All,” Shim and her peers expressed greater optimism than Smith. They examined the concerns like those she expressed and many others, and then they laid out a detailed plan of action that the nation can take to fix a health care system that “is broken.”
“Eliminating health care inequities and advancing health equity are achievable and feasible goals,” they wrote. “Many of the tools needed to reach these goals are already available and need to be fully used. With concerted national efforts and adequate resources, the health care system can be transformed to deliver high-quality, equitable care to all and contribute to the larger societal goal of achieving optimal health for all. We are all in this together.”
Among the recommendations from the committee: They called for the National Institutes of Health and other funders to pour more money into research aimed at addressing health care inequities, structural racism, and health-related social needs. They want to see more health equity studies evaluating the comparative effectiveness of interventions and approaches to implementation rather than simply documenting disparities.
To rebuild trust broken by past discrimination and judgment, they said, involve Black people with lived experience “at every step, from conceptualization to dissemination, and share decision-making power and ownership with the research team.” And, work with them to define — and continually refine — evidence-driven solutions into sustainable best practices that, when appropriate, can be expanded to other sites.
“Many, many studies have shown ... that when people from their own communities are helping to lead and drive research, they often have the solutions to the problem, rather than ... the academic person from a different background,” said Shim, the associate dean of diverse and inclusive education in the UCD School of Medicine.
Gay and bisexual men have faced judgment and stigma in the health care system, from their families and in their faith communities, Flournoy said, so they could bring much-needed perspective on how to build awareness and overcome barriers to adoption of testing and treatments.
“Even for those who practice safe sex with the same person of the same gender, there’s still a stigma,” he said, “so people are not being tested because they don’t want to be identified as being positive or negative for fear of what that would mean in terms of their families, their communities, their jobs, their faith community. People are fearing, alienation and ostracism.”
Black people fear HIV diagnosis will lead to ostracism
Flournoy recalled visiting churches where he recognized men he knew were having sex with other men, and he would see them shout “Amen” when their pastor condemned homosexuality as a sin in his Sunday sermon. Early in his own Christian formation, Flournoy said, he devoted himself to church work and prayed fervently to God to heal him of his attraction to men.
His parents were evangelicals, he said, and when he had told them separately of his struggles with his sexuality, each of them tried to get him to reject his conviction that he might be gay. So, for years after his HIV diagnosis, he delayed telling his parents and other family.
Then, one day in the 1990s, Flournoy said, he, his wife and his mother were having dinner when his mom made clear that she felt HIV and AIDS were God’s judgment on homosexuals. It was a common belief among many Christians at the time — and still holds sway among some.
After that dinner, he decided he could live with HIV, but he could no longer live with his family not knowing he had it. Days later, he called his mother and told her about his diagnosis.
“I do remember apologizing, and saying, ‘I’m so sorry, I shamed the family,’” Flournoy said, “and I think that’s what many African Americans deal with. We believe that to be HIV positive is a source of shame and guilt.”
Flournoy no longer holds such views: HIV has nothing to do with God’s judgment, he said. “It is a biomedical disease.”
When the initial shock of his HIV diagnosis wore off, Flournoy said, he started to get angry.
“I started thinking, ‘I can do something and the God that I serve can do something,’ and I’m not settling for what the nurse said,” Flournoy said. “(HIV) affects us spiritually, socially, emotionally, but there’s so much support out there.”
Flournoy, now an ordained minister, wants people to know that there is life on the other side of an HIV diagnosis. He has worked as a missionary in Africa and as a chaplain in Hawaii. Over his life, he adopted four children and had one biological child.
He advocated for people living with HIV for decades in various government and nonprofit positions, and he currently serves on two state and one county advisory board trying to solve inequities in testing, awareness and treatment of HIV.
Men need to know, for instance, that the risk of contracting HIV increases if they’re having sex with other men, Flournoy said. In Sacramento County, such relationships were the most common source of HIV transmission between 2012 and 2021, making up 52% of newly diagnosed cases, records show. Heterosexual contact, on the other hand, accounted for 25% of HIV cases in Sacramento County, and these cases include a rising tide of heterosexual Black women.
What does U=U mean? It’s good news about HIV
HIV medications can suppress the virus to undetectable levels, and after a person has kept their levels undetectable for six months, the virus is untransmittable.
A global U=U campaign has been sharing this news and attempting to pave the way to end the HIV epidemic.
Despite this campaign and significant work by faith-based organizations to rein in the spread of the disease in the Black community, a veteran advocate for people living with HIV said he and his team suffered a painful loss earlier this year.
Jake Bradley-Rowe, the leader of Sacramento-based Sunburst Projects, and his team offer free HIV testing, support groups, and a variety of other social and mental health services to people living with HIV.
One day in August 2022 when temperatures soared above 100 degrees, Bradley-Rowe and one of his staffers went to check on a young African American client who had been diagnosed with HIV. They found him in his sweltering apartment.
He was incredibly sick, Bradley-Rowe said, with a viral load in the millions per milliliter of blood. He and his staffer called 911 and got him into the hospital. After he was discharged, Bradley-Rowe said, they worked to nurse the young man back to health, often taking him meals, even though their grants did not cover those costs.
The young man’s family in Florida held the religious belief that he was broken because he was gay, Bradley-Rowe said.
“I remember calling his mom. I vividly can remember that I was in my car driving home and the street I was on,” Bradley-Rowe said. “It was a bright, hot day and there was one big cloud in the sky and I … (told) his mom that, if she wanted to see her son alive one more time, she should get on a plane and come to California.”
Her response, as Bradley-Rowe recalled it, was “He made the bed. He’ll lay in it alone,’ and she hung up the phone.
In the end, Bradley-Rowe said, the young man worked hard to get stable enough to return home to his family in February of this year. The Sunburst team learned in April that he had died on March 30.
What you should know about HIV prevention
Test at least once a year if you don’t know the HIV status of your sexual partner or if your partner has HIV. The US Centers for Disease Control said that, by 2028, it would distribute 1 million self-tests that can be used at home.
To reduce your risk of getting HIV, learn how to use condoms correctly every time you have sex.
If you do not have HIV, there’s a medication that can help you avoid getting it. Talk to your health care provider about PrEP. Users take a specific HIV medicine every day or an injectable HIV medicine every two months to reduce the risk of getting HIV through sex or injection drug use. (A shot that lasts six months is expected to be available soon.)
Do you have HIV? Take antiretroviral therapy, or ART, as prescribed by your doctor to suppress the amount of HIV in the blood to the point where a test cannot detect it. If you maintain an undetectable viral load, you will not transmit HIV to your partner through sex.
Were you exposed to HIVin the last 72 hours? Go to an emergency room or consult a doctor within three days of a possible exposure to HIV to get medicines that could prevent an infection. PEP, or post-exposure prophylaxis, should be used only in emergency situations. It is not meant for regular use by people who may be exposed to HIV frequently. To be effective, PEP must be taken daily for 28 days.
How to advocate for yourself in the healthcare system
The California Black Health Network has organized a series of webinars to give African Americans the knowledge, skills, tools and resources to make the health care system work better for them.
Want to participate? Go to the current events tab at www.cablackhealthnetwork.org to sign up now for the second of five sessions with Dr. Glenda Newell-Harris, author of “Focus on Your Best Health.” The first session, covering what patients’ rights are and how to exercise them, is available in the organization’s webinar archive.
“We’re really doing our best to ignite a Black health movement in California,” said Rhonda Smith, the network’s executive director, “so that our community can really feel more empowered to take charge and ownership … (of) their health and wellness.”
