How Our Minds Trick Us Into Overlooking Signs of Dementia
- Oops!Something went wrong.Please try again later.
There is a deceptively simple optical illusion that consistently fools us. The Müller-Lyer illusion consists of two parallel lines, one with fins pointing inward and the other with fins extending outward. The lines are of equal length, yet no matter how many times we measure them, the one with the fins diverging will always appear longer. This tension between what we know conceptually and what we perceive instinctively is built into us and is, I believe, at the heart of the caregiver’s dilemma.
Caregivers may realize their parents or spouses suffer from dementia, but in many cases it does not inhibit them from reacting emotionally and erratically to their patient’s misconduct or delusions. Knowing better does not necessarily make caregivers behave better. I encountered this phenomenon so often (even with well-informed caregivers) that I began to wonder if there wasn’t a neurological component to a family member’s inability to accept the full implications of cognitive impairment.
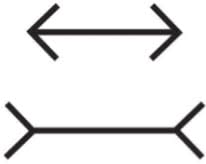
In Thinking, Fast and Slow, the psychologist Daniel Kahneman explains what’s at work here. He postulates two modes of thinking. System 1 is our automatic mode of thinking; it runs effortlessly, forms immediate impressions, and produces visceral and emotional reactions. This unconscious process, which Kahneman dubs “fast thinking,” is almost impossible to suppress. System 1 recruits our intuitions, biases, and assumptions and makes us susceptible to various visual and cognitive pitfalls, such as the Müller-Lyer illusion. System 2 is our more deliberate mode of thinking; it works at a conceptual remove and is slower to pronounce judgment. We can think of System 1 as the loud-mouthed uncle who knows the answer to everything and System 2 as the egghead professor given to murmuring, “I’m afraid I don’t know about that,” or “Maybe we should think things over.” And perhaps if System 2 had more sway over us, it would help us see what we know to be true. Although dementia does not play with lines and angles, it does something even trickier to disguise itself.
On a fall day a few years ago, an experienced social worker came to see me. Jasmine Hines was 36, a tall, pretty, willowy woman with large hazel eyes that often seemed on the verge of welling up. Soft-spoken and even-keeled, she was unflinching when assessing her strengths and weaknesses. She was also honest with others, which helped when dealing with at-risk kids. But after her father, Stewart, died of cancer, she quit her job to take care of her mother, Pat.
When Jasmine spoke about Stewart, her voice brightened with affection and flashes of humor. But when Pat’s name came up, her voice became weary, almost deflated. She often thought about Stewart not just because she missed him, but because she had come to realize how much she had relied on him and how expertly he had hidden Pat’s dementia from her. Even seeing her parents every day, Jasmine never suspected the extent of her mother’s decline.
There’s a Horrifying Link Between Dementia and Car Pollution
Now, looking back, she could identify both subtle and not-so-subtle clues. The time, for instance, that Pat got behind the wheel of her car and turned to Jasmine, saying, “I don’t know what to do here.” To which Jasmine had replied, “Okay, Mom, very funny.” But when Pat opened the glove compartment, a list of instructions on how to start the car fell out. The note was in Stewart’s handwriting.
Jasmine paused, as if to consider what she’d just told me. “That should have tipped me off, huh? Instead I just thought, ‘How convenient. Daddy to the rescue.’”
“Did your father always come to the rescue?” I asked.
“Yes, he did. I should have seen what was happening. But I didn’t want to deal with it, so I ignored it.”
It pained me to see her blaming herself for something that most caregivers also miss. Although clear-cut signs of Alzheimer’s—incoherence, sexual inappropriateness, getting lost in familiar places, paranoid delusions, even physical violence—are often present, family members still hesitate to make the leap to a neurological diagnosis. Patients, of course, don’t need help in denying the disease. How can they keep track of symptoms when they can’t remember things from moment to moment? For so many of them the disease creates and then hides behind cognitive impairment. But what about caregivers? Might not their denial have a neurological component? I believe this to be the case and have come to think of it as “dementia blindness.”
By thinking about it in these terms, I was reminded of the real blind spot that exists in the human eye, at the point where the optic nerve exits the retina. At this one point in each eye there are no photoreceptors. In effect, there is a gap where sensory data is not registered. Nonetheless, when we look out into the world we perceive a complete picture. This is because the brain, using visual information at the borders of the blind spot, fills in the gap with what it expects to see. In a similar way, the brain conceals from us what it doesn’t know with what it does know. It finds our pre-existing emotional blind spot and exploits it.
As I listened to Jasmine, I began to grasp what her blind spot might be. When Stewart was on his deathbed, he had called Pat from the hospital and asked her to bring him a book. Jasmine, who was standing near her mother, saw that Pat was becoming agitated during the call. She didn’t know where the book was, Pat told Stewart. She didn’t know if she could bring it to him. Jasmine was then startled to hear her father yelling over the phone that she had better find the book, and even more startled when Pat became outraged and began to yell back.
Dumbfounded, Jasmine pleaded, “Mom, Dad is dying. He’s allowed to yell at you. When you’re dying, you can do that.”
Hesitantly, I asked Jasmine if she didn’t think that Pat was already suffering from dementia.
She shrugged. “Hey, it was just Mom being Mom.”
Maybe it was just Pat being Pat, but her confusion and anger were also classic signs of dementia. Although it troubled Jasmine that Pat had yelled at Stewart, it didn’t occur to her to consider that her mother’s confusion and anger might signal a neurological problem.
An Injectable Gel Could Zap Your Brain to Treat Alzheimer’s
Once again I saw how hard it is to attribute a neurological cause to the speech and behaviors that have always colored our impressions of people. Caregivers are not just hampered by a patient’s adaptive unconscious, which makes them seem less ill than they are; caregivers’ own minds often misinterpret what’s right in front of them. Patients may unknowingly help create the illusion that they’re still okay, but it is the healthy mind that falls for the illusion. This susceptibility, which often goes unremarked, is fairly common; it might even be likened to the way we’re fooled by an actual optical illusion.
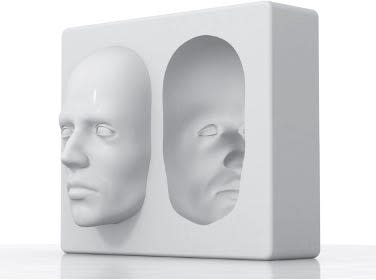
Consider, for instance, the Hollow-Face illusion. We see a convex face even though the lines of the face are actually concave. The face looks convex because our minds have plenty of experience with real faces, which are in fact convex. And this in turn leads to a neural expectation of convexity that is so strong that it trumps the sensory signal (i.e., concavity) itself.
So why does the eye see what the mind knows is wrong? According to the cognitive scientist Andy Clark, these visual mistakes are not glitches in the brain or even random errors. They are, in fact, neural tendencies that reveal something “right” about the brain even if it happens to be, in specific instances, mistaken about what is being viewed.
Traditionally, the perceptual system was believed to be passive or stimulus-driven, a view that reflects our intuitions about reality. We intuitively feel that we have direct access to the outside world and that all we need to do is sit back and let our senses, camera-like, click away. This passive, stimulus-driven view of perception is known as “bottom-up perception.”
Today, however, we know that the brain isn’t just along for the ride; it’s an active participant in perception, and the visible world is the result of a compromise between sensory data and the mind’s expectations based on previous experience. Because we naturally construct an internal model of reality, what we already know influences what is still to be known, if not always accurately. This tendency toward expectation-based perception is referred to as “top-down processing,” and it sometimes causes expectations to override incoming sensory signals. A picture of a face can be concave, but it won’t appear that way to us.
If our expectations can override reality, it’s practically axiomatic that we’ll be fooled by misperceptions more important than an optical illusion. Imagine being in the woods and coming across a bear. If we had no internal model of what woods or bears look like, we’d likely be dead by the time our mind could make sense of the data. Then again, we could be wrong. Perhaps the bear is actually an unusually large, bearish-looking dog. Nonetheless, we’d still think Bear! and run away, or perhaps play dead. Later we might feel embarrassed for overreacting, but it’s a small price to pay. After all, our biological imperative is to survive, not to keep our pride intact or to prevent us from making inconsequential mistakes.
Preconceptions guide us subtly and persuasively. Without an internal model of the world, life would be too noisy, too ambiguous, too chaotic. With nothing to orient us, we’d get lost in endless details, or become confused by too much stimuli, or end up paralyzed by a surfeit of choices. Without experientially shaped expectations, we’d have to start from scratch with every interaction or impression. It would take us too long to figure out what was harmful or benign, who’s a friend or a foe.
So just as memory is not built for accuracy, neither is perception, and the occasional error is surely worth our overall ability to function efficiently. Dementia blindness exists because we do more than merely observe the world around us. We interpret it, as Andy Clark notes, against “a rich background of prior knowledge.” And it’s precisely because we know our spouse or parent so well that dementia tricks us, making us see enough familiar cues to think that everything is fine.
The research of Nassim Nicholas Taleb seems to support this explanation. Taleb argues that we have a propensity to overlook the anomalous by creating “narrative fallacies” that impose coherence by tailoring unexpected phenomena to fit into our preexisting assumptions. In the same way that we make sense of the visual world (which sometimes means being fooled by it), we form expectations of the people around us, projecting narratives onto family members which obscure the evidence of their impairment. We unconsciously smooth out the anomalies dementia presents so that what looks like atypical behavior to an outsider feels like just another familiar assault to a caregiver. And just as we subconsciously impose preconceived expectations on the visual world, causing us to fall for optical illusions, we bend dementia symptoms to fit what we already know about our spouse or parent.
Excerpted from Travelers to Unimaginable Lands. Copyright © 2023 by Dasha Kiper. Published by Random House, an imprint of Penguin Random House.
Get the Daily Beast's biggest scoops and scandals delivered right to your inbox. Sign up now.
Stay informed and gain unlimited access to the Daily Beast's unmatched reporting. Subscribe now.

